Skull base tumours
The part of the skull which forms the bottom of the head is referred to as skull base. The spinal cord, multiple nerves and the major blood vessels of the brain, head and neck pThe part of the skull which forms the bottom of the head is referred to as skull base. The spinal cord, multiple nerves and the major blood vessels of the brain, head and neck pass through openings in the skull base. It is divided into three parts
- Anterior cranial fossa base
- Middle cranial fossa base
- Posterior cranial fossa base
The common malignant skull base tumours are:
- Adenocarcinoma
- Olfactory neuroblastoma
- Carcinoma – Nasopharyngeal, Squamous cell, Mucoepidermoid, Neuroendocrine
- Lymphoma
- Chondrosarcoma
- Chordoma
- Melanoma
- Metastases
- Myeloma/plasma cell tumours
- Sarcomas – Ewings, Osteosarcoma etc
The most common benign skull base tumours include:
- Meningioma
- Schwannomas – Vestibular, trigeminal, Jugular foramen
- Pituitary tumours
- Epidermoid and dermoid cysts
- Craniopharyngiomas
- Paraganglioma
- Cholesteatoma
- Fibro-osseous lesions
- Hemangioma
- Inverting Papilloma
- Lipoma
Malignant head and neck tumours may also extend to the skull base.
Meningioma
Meningiomas are the commonest benign tumours of the brain. Patient can present quite late as these are slow growing tumours. These tumours arise from the meninges of the brain – protective coverings of the brain. There are different types of meningiomas based on the location of the meningiomas.
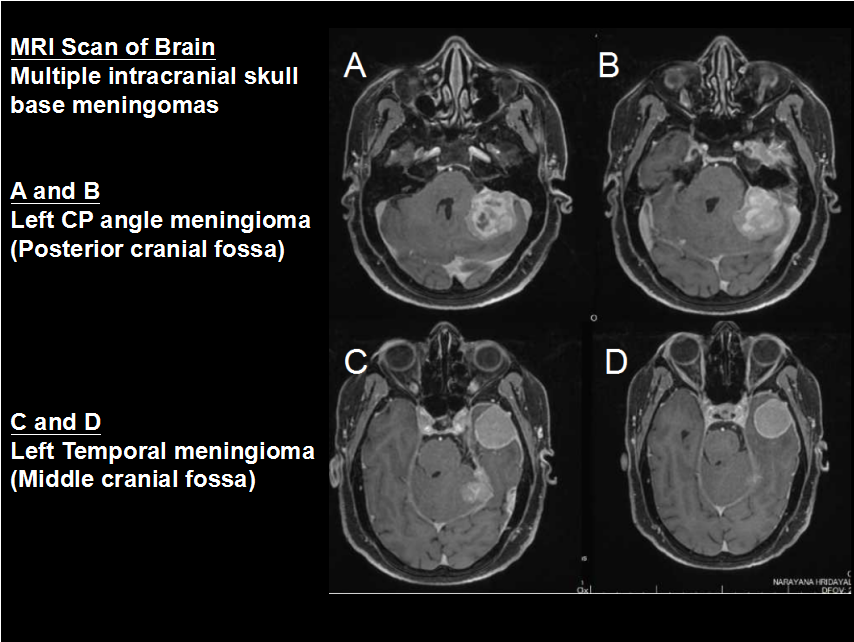
Skull base meningiomas pose a special challenge for the neurosurgeon due to many reasons
-
- Difficult to approach
- Incomplete removal(many a times)
- Resurgery will be challenging
- More vascularity
- Surrounded by vital vascular and neural structures
- More compliacations
Treatment options
Tiny tumours/inoperable tumours : Observation/Fractionated radiotherapy
Accessible tumours : Craniotomy and surgical excision of meningiomas
Residual/high grade tumours : Radiation therapy
Pituitary adenoma and tumours around pituitary gland
The commonest tumour at this location is Pituitary adenoma, followed by craniopharyngioma and Rathkes cleft cyst. Tumours that grow from and around the pituitary gland can affect the whole body by interfering with normal hormone levels. They are commonly seen in young adults. These tumours present with Visual symptoms, hormonal changes along with headache and vomiting. They are diagnosed with the help of imaging modalities like MRI. Endocrine evaluation help in identifying hormonal changes. Visual field show characteristic bitemporal hemianopia.
Treatment Options
Observation: Tiny and slow growing tumours
Medication: Few tumours like prolactinomas can be medically treated with medicines like bromocriptine.
Surgery: Trans-nasal endoscopic surgery, a minimally invasive surgery for these tumours via nose is commonly done. For larger tumours craniotomy is done and tumour is removed.
Radiation: For aggressive and residual or recurrent tumours need radiation therapy
Epidermoid
These are benign and slow growing tumours which arise due to trapping of epidermal cells during development. They slowing grow in size and present with symptoms once they are sizeable. They are usually seen in the base of the skull around the brain stem and the cerebellum.
They are adherent to the neural and vascular structures. Radical/Total surgical excision is the treatment of choice.
Schwannoma
Schwannomas are tumours that grow from the sheath covering the nerves. They are benign tumours and grow slowly. The commonest schwannoma is the one arising from vestibular nerve, the nerves responsible for balance and hearing – called, Vestibular Schwannoma.
Symptoms: The tumour can cause gradual hearing loss, ringing in the ear, dizziness and imbalance while walking. Large tumours can cause weakness of facial muscles and also one side of the body.
Diagnosis: MRI shows the extent of the tumour in the CP angle, also its extension into the narrow compartments around the brain stem. Audiometry will throw more light on
Treatment: Because of their slow growth, not all acoustic neuromas need to be operated. Treatment options include observation, surgery, and radiosurgery.
Observation – tiny tumours, especially intracanalicular or those in the elderly or bilateral small tumours, in a patient with type II NF
Surgery – The classical suboccipital restromastoid craniectomy and tumour excision would be the preferred approach by many neurosurgeons.
Radiosurgery – for small tumours and the residual tumours, Gamma knife radiosurgery and SRS offer good results.ass through openings in the skull base. It is divided into three parts
Anterior cranial fossa base
Middle cranial fossa base
Posterior cranial fossa base
The common malignant skull base tumours are:
- Adenocarcinoma
- Olfactory neuroblastoma
- Carcinoma – Nasopharyngeal, Squamous cell, Mucoepidermoid, Neuroendocrine
- Lymphoma
- Chondrosarcoma
- Chordoma
- Melanoma
- Metastases
- Myeloma/plasma cell tumours
- Sarcomas – Ewings, Osteosarcoma etc
The most common benign skull base tumours include:
- Meningioma
- Schwannomas – Vestibular, trigeminal, Jugular foramen
- Pituitary tumours
- Epidermoid and dermoid cysts
- Craniopharyngiomas
- Paraganglioma
- Cholesteatoma
- Fibro-osseous lesions
- Hemangioma
- Inverting Papilloma
- Lipoma
Malignant head and neck tumours may also extend to the skull base.
Meningioma
Meningiomas are the commonest benign tumours of the brain. Patient can present quite late as these are slow growing tumours. These tumours arise from the meninges of the brain – protective coverings of the brain. There are different types of meningiomas based on the location of the meningiomas.
Skull base meningiomas pose a special challenge for the neurosurgeon due to many reasons
-
- Difficult to approach
- Incomplete removal(many a times)
- Resurgery will be challenging
- More vascularity
- Surrounded by vital vascular and neural structures
- More compliacations
Treatment options
Tiny tumours/inoperable tumours : Observation/Fractionated radiotherapy
Accessible tumours : Craniotomy and surgical excision of meningiomas
Residual/high grade tumours : Radiation therapy
Pituitary adenoma and tumours around pituitary gland
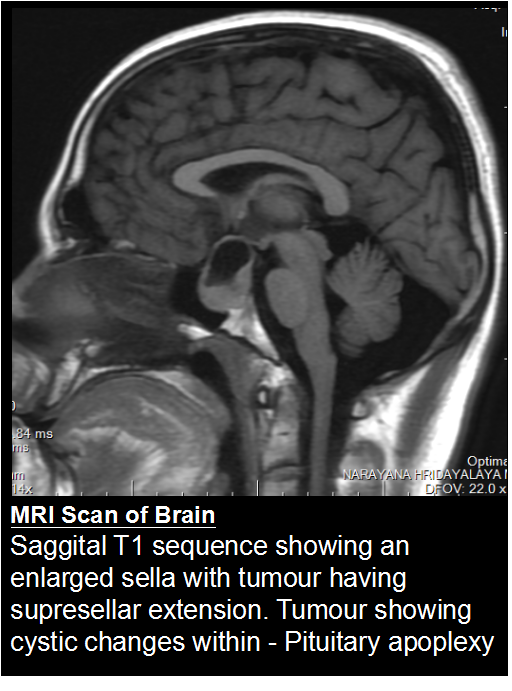
The commonest tumour at this location is Pituitary adenoma, followed by craniopharyngioma and Rathkes cleft cyst. Tumours that grow from and around the pituitary gland can affect the whole body by interfering with normal hormone levels. They are commonly seen in young adults. These tumours present with Visual symptoms, hormonal changes along with headache and vomiting. They are diagnosed with the help of imaging modalities like MRI. Endocrine evaluation help in identifying hormonal changes. Visual field show characteristic bitemporal hemianopia.
Treatment Options
Observation: Tiny and slow growing tumours
Medication: Few tumours like prolactinomas can be medically treated with medicines like bromocriptine.
Surgery: Trans-nasal endoscopic surgery, a minimally invasive surgery for these tumours via nose is commonly done. For larger tumours craniotomy is done and tumour is removed.
Radiation: For aggressive and residual or recurrent tumours need radiation therapy
Epidermoid
These are benign and slow growing tumours which arise due to trapping of epidermal cells during development. They slowing grow in size and present with symptoms once they are sizeable. They are usually seen in the base of the skull around the brain stem and the cerebellum.
They are adherent to the neural and vascular structures. Radical/Total surgical excision is the treatment of choice.
Schwannoma
Schwannomas are tumours that grow from the sheath covering the nerves. They are benign tumours and grow slowly. The commonest schwannoma is the one arising from vestibular nerve, the nerves responsible for balance and hearing – called, Vestibular Schwannoma.
Symptoms: The tumour can cause gradual hearing loss, ringing in the ear, dizziness and imbalance while walking. Large tumours can cause weakness of facial muscles and also one side of the body.
Diagnosis: MRI shows the extent of the tumour in the CP angle, also its extension into the narrow compartments around the brain stem. Audiometry will throw more light on
Treatment: Because of their slow growth, not all acoustic neuromas need to be operated. Treatment options include observation, surgery, and radiosurgery.
Observation – tiny tumours, especially intracanalicular or those in the elderly or bilateral small tumours, in a patient with type II NF
Surgery – The classical suboccipital restromastoid craniectomy and tumour excision would be the preferred approach by many neurosurgeons.
Radiosurgery – for small tumours and the residual tumours, Gamma knife radiosurgery and SRS offer good results.
GENERAL ENQURIES
186 0208 0208
+91 8884415615 | +91 8884458890
- gouthamcugati@gmail.com
- Narayana Multispecialty Hospital.
CAH/1, 3rd Phase, Devanur, Ring Road,
Mysore – 570019
OFFICE HOURS
| Monday – Saturday | 09:00 AM – 5:00 PM |