Brain tumours
A brain tumour is an abnormal growth of cells inside the brain or skull, due to uncontrolled multiplications of cells. Some are benign (non cancerous), others are malignant (cancerous). Tumours can grow from the brain tissue itself (primary brain tumour), or tumour from other places in the body spreading to the brain (metastasis). Treatment options vary depending on the tumour type, size and location.
Types of Primary brain tumours
- Gliomas
- Astrocytoma
- Glioblastoma Multiforme (grade IV)
- Oligodendroglioma
- Ependymoma
- Meningioma
- Pituitary adenoma and tumours around pituitary gland
- Epidermoid
- Lymphoma
- Schwannoma
- Pineal region tumours
- Medulloblastoma
Causes of brain tumours
There is no known cause of brain tumours. There are a few subset of people who can be at risk for brain tumours. They are
1.Tumour elsewhere in the body
- Genetic disorders like P53 gene deletion
- Exposure of chemicals or solvents
Symptoms of brain tumour
- Headache
- Vomiting
- Visual blurring
- Speech disturbances
- Weakness or numbness of one side of the body
- Unsteadiness of gait, dizziness, hearing disturbance
- Drowsiness, unconsciousness or fits
Diagnosis
CT Scan: Computerised Tomography is a diagnostic modality which used X-ray beam to visualise the brain structure.
MRI Scan : Uses magnetic field and radiofrequency waves to visualise the brain structure.
Blood Investigations : Endocrine and harmonal evaluation
Lumbar Puncture
Visual and auditory assessment
Histopathological examination of the tumour, which is removed by surgery or biopsy is the gold standard to check for the grades of the tumour.
Treatment Options
The treatment of the brain tumours depend on location, size, type of the tumour and also the characteristics of the tumours on the imaging
- Observation – Usually small, benign, slow growing tumours are observed over a period of time with serial imaging.
- Medications -Anticonvulsants to prevent seizures Mannitol, steroids and lasix to reduce the swelling and protect the brain
- Surgery – Surgery is the treatment of choice for majority of the brain tumours. The part of the skull is removed(craniotomy) and the tumour is removed from the brain while protecting the surrounding brain. Depending on the location of the tumour, appropriate craniotomy is planned by the neurosurgeon.
- Radiation Therapy – If the tumour is cancerous, most of the times, radiation and chemotherapy might be required. Radiation therapy is modality where high energy X rays or gamma rays are used to destroy he aggressive tumour cells by preventing their multiplication.
- Chemotherapy -Chemotherapy is a modality where drugs are used to prevent rapid multiplication of the tumour cells.
Gliomas
Gliomas are primary brain tumours, which grow from the brain parenchyma and requires surgery.
Gliomas can be
-
- Astrocytoma
- Glioblastoma Multiforme (grade IV)
- Oligodendroglioma
- Ependymoma
There are different grades of the tumour like Grade I, II,III,IV and Glioblastoma Multiforme.
If the tumour is of higher grade then adjuvant Chemo-radiation will be required after surgery

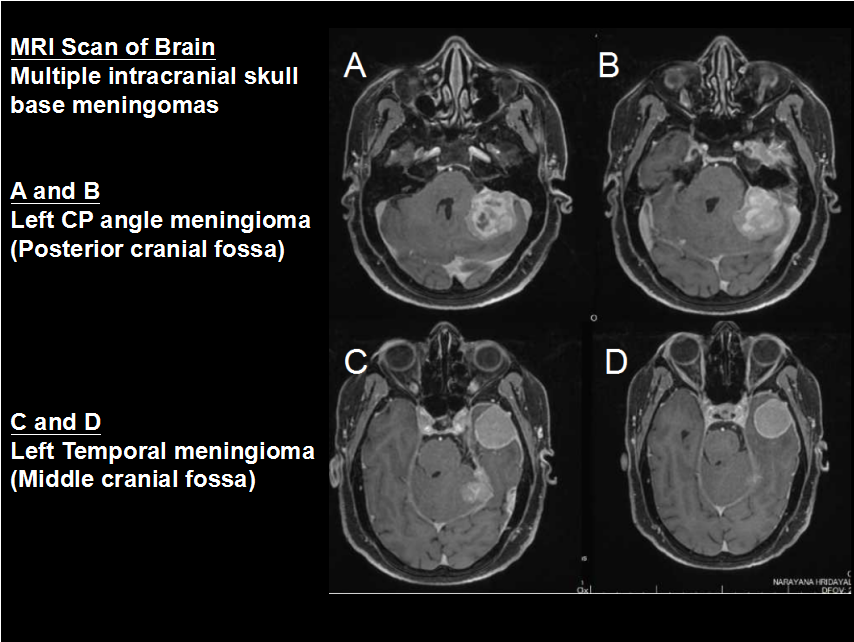
Meningioma
Meningiomas are the commonest benign tumours of the brain. Patient can present quite late as these are slow growing tumours. These tumours arise from the meninges of the brain – protective coverings of the brain. There are different types of meningiomas based on the location of the meningiomas.
Treatment options
Tiny tumours/inoperable tumours : Observation/Fractionated radiotherapy
Accessible tumours : Craniotomy and surgical excision of meningiomas
Residual/high grade tumours : Radiation therapy
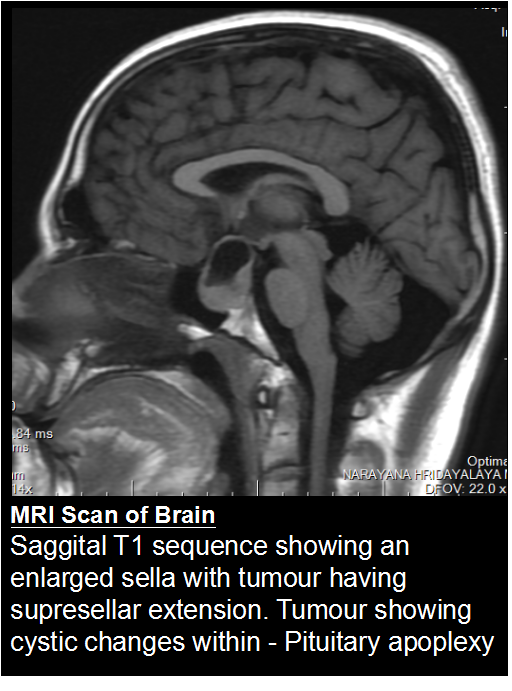
Pituitary adenoma and tumours around pituitary gland
Tumours that grow from and around the pituitary gland can affect the whole body by interfering with normal hormone levels. The commonest tumour at this location is Pituitary adenoma, followed by craniopharyngioma and Rathkes cleft cyst. They are commonly seen in young adults. These tumours present with Visual symptoms, hormonal changes along with headache and vomiting. They are diagnosed with the help of imaging modalities like MRI. Endocrine evaluation help in identifying hormonal changes. Visual field show characteristic bitemporal hemianopia.
Treatment Options
Observation: Tiny and slow growing tumours
Medication: Few tumours like prolactinomas can be medically treated with medicines like bromocriptine.
Surgery: Trans-nasal endoscopic surgery, a minimally invasive surgery for these tumours via nose is commonly done. For larger tumours craniotomy is done and tumour is removed.
Radiation: For aggressive and residual or recurrent tumours need radiation therapy
Epidermoid
These are benign and slow growing tumours which arise due to trapping of epidermal cells during development. They slowing grow in size and present with symptoms once they are sizeable. They are usually seen in the base of the skull around the brain stem and the cerebellum.
They are adherent to the neural and vascular structures. Radical/Total surgical excision is the treatment of choice.
Primary Intracranial Lymphoma
These are aggressive form of lymphomas, which are malignant and have poor prognosis. MRI/CT Scan shows multiple periventricular lesions in the brain. Once diagnosis of lymphoma is made either by biopsy or surgical excision, the main stray of treatment is chemotherapy with or without radiation.
Schwannoma
Schwannomas are tumours that grow from the sheath covering the nerves. They are benign tumours and grow slowly. The commonest schwannoma is the one arising from vestibular nerve, the nerves responsible for balance and hearing – called, Vestibular Schwannoma.
Symptoms: The tumour can cause gradual hearing loss, ringing in the ear, dizziness and imbalance while walking. Large tumours can cause weakness of facial muscles and also one side of the body.
Diagnosis: MRI shows the extent of the tumour in the CP angle, also its extension into the narrow compartments around the brain stem. Audiometry will throw more light on
Treatment: Because of their slow growth, not all acoustic neuromas need to be operated. Treatment options include observation, surgery, and radiosurgery.
Observation – tiny tumours, especially intracanalicular or those in the elderly or bilateral small tumours, in a patient with type II NF
Surgery – The classical suboccipital restromastoid craniectomy and tumour excision would be the preferred approach by many neurosurgeons.
Radiosurgery – for small tumours and the residual tumours, Gamma knife radiosurgery and SRS offer good results.
Pineal region tumours
The tumours in the pineal gland are collectively called pineal region tumours. The pineal gland is considered the third eye of the human body which regulates many aspects of the human body like, hunger, sex, sleep(circadian rythms), thirst and also the biological clock. The commonest tumours being the germ cell tumours, pinealocytoma, pinealoblastoma. Patients usually present with hydrocephalus, seizures. MRI Scan is helpful in the identification of the tumours. Tumour markers help in isolating, germ cell tumours. Teratomas can be treated with medicines, however all other tumours need surgery. Some may need chemoradiation post surgery.
Medulloblastoma
These are the commonest tumours in the children. They occur in midline in the posterior fossa. They are malignant tumours and often have poor prognosis. The children commonly present with weakness of lower limbs, gait imbalance, drowsiness and in advanced cases cranial nerve involvement can be seen. Surgery is the mainstream of treatment. Following surgery, chemotherapy and cranio-spinal irradiation will be required.
GENERAL ENQURIES
186 0208 0208
+91 8884415615 | +91 8884458890
- gouthamcugati@gmail.com
- Narayana Multispecialty Hospital.
CAH/1, 3rd Phase, Devanur, Ring Road,
Mysore – 570019
OFFICE HOURS
| Monday – Saturday | 09:00 AM – 5:00 PM |